
Hope Amid a Continuing Crisis

It’s been 20 years since her doctor silently handed Katrina Robertson a lab report that showed she was infected with human immunodeficiency virus (HIV). Yet the memory is still painfully fresh.
“I remember just boo-hooing and crying because it was like I’m gonna die,” said the 47-year-old native Nashvillian. “Everybody I’d heard about … it was an immediate death sentence.”
HIV affects specific cells of the immune system, and over time, it can destroy so many of these cells that the body can’t fight off infections and disease, resulting in acquired immune deficiency syndrome—AIDS.
With a positive HIV test, Robertson, who’d struggled with devastating drug addiction for years, relapsed. “I couldn’t stay clean,” she said. “I thought if I was going to die anyway I might as well kill myself. But God had another plan for me.”
Fortuitously, around the same time as Robertson’s diagnosis, new, more effective drugs that blocked HIV replication reached the market, and the Comprehensive Care Center (CCC), Nashville’s first medical “home” for people infected with HIV, had opened the previous year.
Family nurse practitioner Beverly Byram, M.S.N., R.N., however, remembers the terribly sick and incredibly brave young men and a few young women who passed through the CCC before there was effective treatment for AIDS.
One man had been in hospice for several weeks when he made an appointment to see Byram. He handed her a paperweight his grandmother had given to him. On the bottom he’d taped the photo from his driver’s license. “Don’t ever forget me,” he said. He died the next day.
“I think about him often,” Byram said. “The paperweight is in my office on a shelf of other mementos. I look at them every day to remind me why I’m here.”
Stephen Raffanti, M.D., MPH, medical director of what is now the Vanderbilt Comprehensive Care Clinic (VCCC), remembers breaking into an apartment to rescue a patient with AIDS and severe schizophrenia who’d missed several appointments.
Raffanti and two nurses found the man lying in filth, abandoned. They took him to the home of two gay men who cared for him until he died four months later. “He told me they were the happiest four months of his life,” Raffanti recalled.
This was the era of AIDS after the discovery in 1983 of HIV, which hijacks and disables a critical part of the body’s immune defenses, but before the mid-1990s, when anti-retroviral drugs that prevent HIV from replicating itself became available.
Almost overnight the new drugs transformed HIV infection from a virtual death sentence into a manageable, chronic disease—at least in resource-rich countries like the United States. Yet the battle against AIDS is far from over, and it still could be lost.
Doubling the risk
AIDS remains a major killer in parts of the world where access to effective treatment is limited. Even in this country, 50,000 new HIV infections occur annually, and long-term survivors face serious health challenges, notably a doubling of the risk of heart attacks and strokes.
“We really need better ways to reverse the epidemic. Without research, that’s not going to happen,” said David Haas, M.D., who leads the clinical research effort at Vanderbilt University Medical Center to improve HIV treatment.
“Without a vaccine, it will be very hard to ever really control it,” added Barney Graham, M.D., Ph.D., who, as a Vanderbilt chief resident in 1982 diagnosed one of the first two cases of AIDS in Tennessee. “It’s going to require another breakthrough.”
Graham, a former professor of Medicine at Vanderbilt, is deputy director of the Vaccine Research Center at the National Institute of Allergy and Infectious Diseases, part of the National Institutes of Health (NIH). He and his colleagues are closing in on HIV.
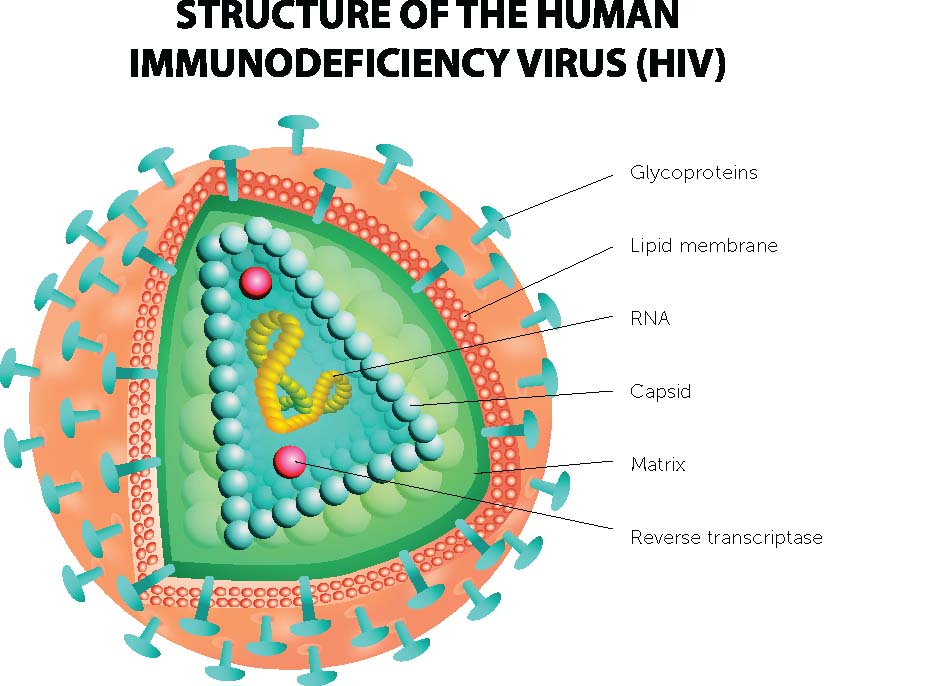
They and others have discovered that the viral envelope protein, the outer coating that the immune system “sees” and which antibodies target, is hypervariable, constantly changing. It’s also flexible, covered with sugars, and presents a decoy to antibodies to throw them off the chase.
Since 2009, however, researchers at NIH and around the country have developed hundreds of monoclonal antibodies capable of neutralizing HIV.
These are antibodies generated in the laboratory against specific targets by selecting B cells using specially designed probes and recovering the immunoglobulin genes from individual cells in order to synthetically produce the antibodies made by that cell.
The resulting “guided missiles” have helped researchers map the vulnerable sites on the HIV envelope. This is aiding efforts, at NIH, Vanderbilt and elsewhere, to develop the first effective vaccine against the virus.
It also may be possible, Graham said, to inject neutralizing antibodies (instead of vaccinating) as a way to prevent HIV infection from taking hold in people who have been exposed to the virus.

At Vanderbilt, James Crowe Jr., M.D., director of the Vanderbilt Vaccine Center, and Jens Meiler, Ph.D., associate professor of Chemistry and Pharmacology, have taken this line of research to another level.
With the help of a computer program that predicts the structure of a protein from its amino acid sequence, they and their colleagues have redesigned an antibody so that it has increased potency and can neutralize more strains of HIV than the original natural antibody.
Their findings, reported in May in the Journal of Clinical Investigation, suggest that computer-redesigned antibodies may speed the search for a curative therapy or vaccine for a virus that so far has eluded all attempts to eradicate it.
“If computational design … can predict how viruses evolve in the future, we could potentially design antibodies and vaccines for viruses before they occur in nature,” said Crowe, the Ann Scott Carell Professor and professor of Pediatrics, and of Pathology, Microbiology and Immunology.
Kick-and-kill
Haas, who has directed the Vanderbilt HIV Therapeutics Clinical Research Site since 1996, is involved in a multi-center study aimed at draining the body of latent reservoirs of HIV that hide out in quiescent white blood cells.
The strategy, called kick-and-kill, involves selective activation of virus in the dormant cells while the patient is on HIV therapy. The hope is that the cells will either die or be recognized and killed by the immune system.
Another multi-center study is testing whether giving HIV patients a statin will reduce their risk of heart attacks and strokes. Statins not only lower cholesterol, but reduce chronic inflammation, a risk factor for blood vessel disease that also is associated with HIV infection.
The Therapeutics Clinical Research Site (CRS) is one arm of Vanderbilt’s AIDS Clinical Trials Unit. The other is the Vanderbilt HIV Vaccine Program, directed by Spyros Kalams, M.D., associate professor of Medicine.
Vanderbilt also is a partner in the recently established Tennessee Center for AIDS Research with Meharry Medical College and the Tennessee Department of Health. The center’s aims are twofold: to improve the continuum of HIV/AIDS care in Tennessee and beyond, and to advance personalized care in the treatment of HIV.
Personalized care is “a huge strength” at Vanderbilt, Haas said. It refers not only to genetic variations that may affect patients’ response to medications, but to other important medical, social and environmental factors that impact the course of disease including AIDS.
The new center will draw from the Vanderbilt Institute of Global Health, which has helped to pioneer the continuum of HIV care in countries like Mozambique, as well as from the VCCC.
“We have the opportunity to take what’s been learned there and bring it to the United States,” Haas said.
The Tennessee Center for AIDS Research investigators are involved in small pilot and large multicenter projects aimed at preventing long-term complications of chronic HIV infection, including heart disease and stroke, pursuing potential treatments that could one day lead to a cure for the disease, and developing an effective vaccine to prevent HIV infection.
The need is great, and much work remains to be done but, said Haas, “we’re getting closer.”
 HIV may not yet be subdued, but 30 years of fighting has helped win other battles – against hepatitis C and RSV, respiratory syncytial virus, for example.
HIV may not yet be subdued, but 30 years of fighting has helped win other battles – against hepatitis C and RSV, respiratory syncytial virus, for example.
And yet, because of a decade of flat federal funding for biomedical research, “I think we’ve lost two generations of physician-researchers,” Graham said. “The barriers to establishing a laboratory or doing research are so high (that) they’re not going to choose research.
“What’s going to happen in the future when we don’t have the workforce or resources to address new problems that come up?”
Today, Katrina Robertson, whose future appeared bleak 20 years ago, is the national sales director for Thistle Farms, a Nashville-based residential program and social enterprise run for and by women who have survived lives of prostitution, trafficking, addiction and life on the streets.
Robertson, who’s been in recovery for 10 years, is enjoying a full life that includes her husband, Barry, and daughter, Ebony.
She continues to receive treatment at the VCCC. “I take good care of myself,” she said. “I eat right. I exercise. I take my medicine. I work closely with my doctor. We can live normal healthy lives.”
Yet she worries that shame, guilt and stigma still keep many people from being tested or seeking treatment. “We’ve got to talk about it … and help people understand it’s not a death sentence anymore and see that we live long, healthy and happy lives and to understand the importance of getting treatment.”